Mass spectrometry & spectroscopy
Published over 6 years ago. See the latest and most current information on Mass spectrometry & spectroscopy.
Mass spectrometry (MS) imaging is a well-established yet still growing technique used to gain insights into the spatial distribution of molecules in a range of samples. The list of applications continues to expand but MALDi Imaging has made a significant impact in the fields of metabolomics, proteomics, biomarker discovery and, more recently, clinical proteomics. MALDI Imaging is now recognised as the go-to technique for untargeted, label-free investigations of metabolites, proteins, peptides, lipids and glycans, where thousands of molecules may be imaged in one run.
While there are many ionisation methods used for MS imaging, matrix-assisted laser desorption/ionisation (MALDI) has emerged as a powerful tool for mapping the distribution of molecules in thin samples. Its capacity to measure a wide range of molecules, from small metabolites to large proteins, has contributed to its rise in popularity. MALDI Imaging is the only proteomic technology that enables detailed assignment of detected biomarkers to histological features, making it ideally suited to correlate molecular signals to clinical end-points i.e., tissue typing, particularly for diseases such as cancer.
Despite this potential, MALDI Imaging is yet to be widely accepted for clinical analysis. For the technology to successfully transfer from a research platform to a universally accepted clinical diagnostic tool, a standardised procedure should be established and followed. Many diseases are heterogeneous, not only between patients but at the molecular level within one patient tissue sample, so biomarker development relies on the analysis of large sample cohorts, which in turn requires highly reproducible methods. The translation of MALDI Imaging into clinical pathology has the potential to drive personalised approaches to treatments and improve disease monitoring, so the focus has turned towards standardisation and reproducibility of these workflows.
Many features of MALDI Imaging technology make it ideally suited for clinical pathology applications. For example, biomarker discovery protocols can utilise fresh-frozen or formalin-fixed paraffin-embedded (FFPE) tissue sections, or tissue microarrays (TMAs). Fresh frozen tissue is not widely available in most routine diagnostic settings, so FFPE tissues are often used for traditional histopathological applications as they are routinely collected during hospital care. Hence, large tissue bank collections of FFPE tissues are available for clinical research of large patient cohorts. FFPE specimens also maintain excellent tissue morphology and allow the direct collection of both spatial and molecular information. Another benefit of this tissue acquisition method is that it does not require target-specific reagents, such as antibodies, making MALDI Imaging of FFPE samples an ideal biomarker discovery tool.
In traditional LC-MS/MS analyses of FFPE tissues, large sample sizes are required, which is impractical in the clinical setting. Sample preparation procedures for this method are also prone to loss of spatial information. MALDI Imaging experiments, however, retain spatial distribution by detecting multiple molecules in a single intact tissue section. Such experiments include tissue typing, where tissue or clinically specific molecular profiles are created. The label-free and non-destructive nature of MALDI Imaging makes it an ideal technique for preserving tissue material for subsequent analyses, for example with cancer biopsies.
Another advantage of MALDI Imaging is the direct analysis of tissues, which does not require the time-consuming step of sample homogenisation – often leading to loss of sample – that is needed to overcome the issue of molecular heterogeneity.
Despite the benefits of MALDI imaging for proteomic analysis, there are relatively few large scale studies providing evidence of the reliability of this technology for clinical applications. There is a need for validation studies to bring the measurement of new marker molecules through to clinical implementation, but the variability of results between different laboratories currently restricts its clinical use. To bridge this gap, a recent reproducibility study investigated whether several laboratories across different geographical locations could achieve reproducible results using standardised sample preparation methods and MALDI Imaging workflow [1].
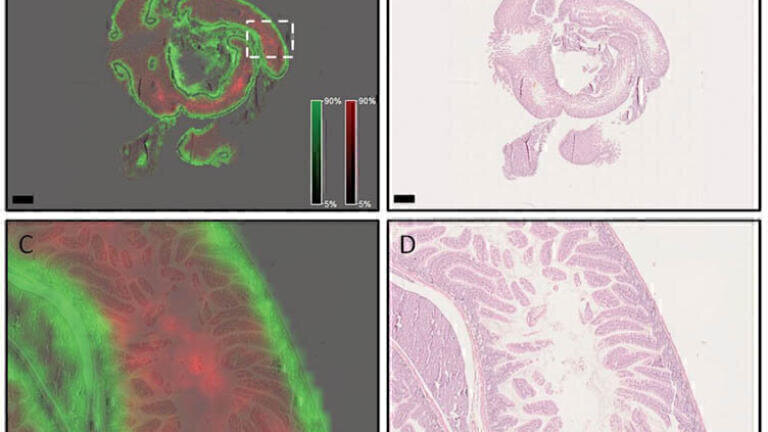
The in situ tryptic peptide digestion procedure for MALDI Imaging was developed to preserve spatial resolution while minimising preparation time and improving reproducibility. Specific m/z features were detected in discrete histological features in mouse intestine, human ovarian teratoma, and human squamous cell carcinoma of the lung. Two different m/z values were localised in FFPE mouse intestine with distinct distributions using a rapifleX MALDI Tissuetyper (Figure 1A) and when correlated with hematoxylin and eosin (H&E) stained samples (Figure 2B), m/z 944.6 was found to be primarily localised in the intestinal villi and lumen, and m/z 1105.6 in the crypts and underlying muscular layers.
Figure 1. Spatial distributions of different m/z species are highly conserved in FFPE mouse intestine sample prepared with reported sample preparation protocol. A) Overview of mouse small intestine showing m/z 944.6 (red) in the villi and lumen, while m/z 1105.6 (green) is primarily in the crypts and muscle layers. Scale bar indicates 1 mm. B) Post-measurement H&E stained sample. Scale bar indicates 1 mm. Higher magnification images (area denoted in [A] with white dotted box) of the m/z species (C) and H&E (D) overlay confirm the distributions. Scale bars indicate 100 μm. Reproduced with permission from reference [1] under https://creativecommons.org/licenses/by/4.0/.
Although trypsin application and digestion are known to be sources of variation and loss of spatial resolution in MALDI Imaging of FFPE samples, the standardised workflow could discriminate discrete histological features in different tissues, enabling different sample sites to generate similar quality images.
Following the confirmation that spatial resolution could be maintained, the study examined the reproducibility of MALDI Imaging results across a multicentre investigation. The approach was two-fold: (1) can different operators perform the same experiment in different laboratories and obtain similar results, and (2) can similar data be obtained from different tissue sources? While it is not possible for users to obtain identical results due to inherent differences between samples, the multicentre study found that the greatest source of variation was due to biology within the tissue, rather than sampling location or time and site of preparation. This shows that if laboratories adhere to stringent MALDI Imaging workflows, reproducibility is possible. The ultra-high-speed of modern MALDI time-of-flight (TOF) mass spectrometry instrumentation facilitates this translation into the clinical research setting. For example, in this study a 4 mm diameter tissue sample could be measured in 6 minutes, at an acquisition rate of 40 pixels per second.
Reproducibility studies such as the one described are relevant to other clinical pathology techniques. Digital polymerase chain reaction (dPCR) is commonly used to reliably detect genetic mutations, and its combination with MALDI Imaging has great potential for patient stratification. One study investigated the use of dPCR following MALDI Imaging analysis of FFPE tissue sections to distinguish between two major subtypes of non-small cell lung cancer (NSCLC) – pulmonary adenocarcinoma (ADC) and squamous cell carcinoma (SqCC), to better inform chemotherapy treatment [2].
After MALDI Imaging was completed, tissue samples were tested with dPCR for the known mutations in epidermal growth factor receptor (EGFR) for the molecular diagnosis of ADC, and KRAS proto-oncogene (KRAS), which is the most frequently mutated oncogene in lung cancer. The results showed that driver gene mutations could be detected in samples formerly analysed with MALDI Imaging. The ability to carry out MALDI Imaging and dPCR analyses from the same tissue section is highly advantageous, as biopsy material is often limited. This combination of proteomic and genetic analysis in one workflow is made possible by the non-invasive nature of MALDI Imaging, which has shown to maintain DNA quality for subsequent analysis by techniques such as dPCR.
In addition to dPCR, other studies have confirmed the combined power of MALDI Imaging and immunohistochemistry (IHC). Results from one experiment showed the co-localisation of specific peaks with ADC (m/z 943.53) and SqCC (m/z 1410.62) [3], which have previously been identified as HistoneA2 and CK5 by MS/MS analysis [4, 5, 6]. The quality of IHC staining after MALDI Imaging was adequate to perform accurate data extraction from regions of interest (ROI) and identify cells of interest. The study also displayed the viability of double IHC stains after MALDI Imaging analysis, which is a useful tool for subtyping of cell populations, for example from biopsies, and protein information can be matched without additional depletion of tissue.
MALDI Imaging is increasingly used to distinguish the molecular signature of different cancers. A retrospective collaborative study analysed 252 FFPE clinical samples from 11 countries to determine whether MALDI Imaging could help classify atypical Spitzoid neoplasms (ASN) [7]. ASN is not a well-defined diagnosis and cases cannot currently be categorised nor clinical behaviour predicted using histopathology. Samples were assigned to four clinical groups, and the study found a strong association between diagnosis of ASN by MALDI Imaging and clinical group, providing a better predicted clinical outcome than histopathology.
Imaging glycans with MALDI Imaging is another approach being investigated to help characterise and distinguish cancers. Glycosylation is a common post-translational modification (PTM) which can be detected with MS, but there are almost no commercially available antibodies, making their spatial examination almost impossible. One study used a newly developed MALDI Imaging method to spatially profile N-linked glycans in human breast cancer FFPE tissue sections and tissue microarrays (TMA) [8]. There are many sub-types of breast cancer with distinct biological features and clinical presentations, which are classified based on the expression status of hormone receptors and human epidermal growth factor receptor 2 (HER2). Early characterisation of these sub-types is crucial to provide timely, appropriate treatment. Researchers could use MALDI Imaging to detect the presence of multiple polylactosamine N-glycans in HER2+, triple-negative and metastatic breast cancers. This information could be used to improve understanding of how breast cancer develops and spreads, to inform clinical biomarker development and ultimately support diagnosis, prognosis and treatment.
Another study established a tissue-based MALDI Imaging method to obtain relative abundance and spatial distribution information of N-glycans in hepatocellular carcinoma (HCC) [9]. The method identified 10 glycans that were significantly increased in the HCC TMA samples, which could be divided into two major classes: those with increased fucosylation and those without fucosylation, but with increased branching. It is hoped that these glycan alterations can be used to detect HCC earlier and improve treatment options.
For MALDI Imaging to be implemented in wide-scale clinical research applications, including diagnostics and prognostics, it must be able to generate reproducible results from samples collected at different locations, by different users, and from different tissue sites. The utility of MALDI Imaging in the diagnosis and treatment of cancer has been demonstrated, for example in the differentiation between ADC and SqCC of the lung, which was previously challenging using traditional IHC techniques, and in the use of MALDI for glycan imaging. MALDI Imaging has the capacity to inform researchers and, potentially, clinicians, of the underlying molecular events driving tumour progression and susceptibility to treatment. Phenotypic differences can be elucidated and markers established to differentiate between otherwise identical tumours, leading to more precise treatment options and a personalised medicine approach.
The continuing development of mass spectrometers, particularly improvements in spatial resolution, sensitivity and sample throughput, is opening up the field of MALDI Imaging to clinical research pathology. The speed and robustness of modern, advanced mass spectrometers allow large specimens to be analysed quickly over large patient cohorts with good spatial resolution, which is crucial for driving this technique forward in diagnostics, prognosis and monitoring treatment responses. The multicentre reproducibility study highlights the need and the real potential for highly standardised sample preparation protocols and MALDI Imaging workflows to build up the data necessary for clinical validation and implementation.
For more information on Bruker’s MALDI Imaging solutions, please visit https://www.bruker.com/applications/life-sciences/maldi-imaging/maldi-imaging-technologies.html.
1. Ly A, Longuespée R, Casadonte R, Wandernoth P, Schwanborn K, Bollwein C, Marsching C, Kriegsmann K, Hopf C, Weichert W, Kriegsmann J, Schirmacher P, Kriegsmann M, and Deininger SO (2019) Site-to-Site Reproducibility and Spatial Resolution in MALDI-MSI of Peptides from Formalin-Fixed Paraffin-Embedded Samples, Proteomics – Clinical Applications, 13, 1800029.
2. Kazdal D, Longuespée R, Dietz S, Casadonte R, Schwamborn K, Volckmar AL, Kriegsmann J, Kriegsmann K, Fresnais M, Stenzinger A, Sültmann H, Warth A, and Kriegsmann M (2018) Digital PCR after MALDI mass spectrometry imaging to combine proteomic mapping and identification of activating mutations in pulmonary adenocarcinoma, Proteomics – Clinical Applications, 13, 1800029.
3. Kriegsmann K, Longuespée R, Hundemer M, Zgorzelski C, Casadonte R, Schwamborn K, Weichert W, Schirmacher P, Harms A, Kazdal D, Leichsenring J, Stenzinger A, Warth A, Fresnais M, Kriegsmann J and Kriegsmann M (2018) Combined Immunohistochemistry after Mass Spectrometry Imaging for superior spatial information, Proteomics – Clinical Applications, doi:10.1002/prca.201800035.
4. Kriegsmann M, Casadonte R, Kriegsmann J, Dienemann H, Schirmacher P, Kobarg JH, Schwamborn K, Stenzinger A, Warth A and Weichert W (2016) Reliable Entity Subtyping in Non-small Cell Lung Cancer by Matrix-assisted Laser Desorption/Ionization Imaging Mass Spectrometry on Formalin-fixed Paraffin-embedded Tissue Specimens, Molecular & Cellular Proteomics, 15(10):3081-3089.
5. Djidja MC, Claude E, Snel MF, Francese S, Scriven P, Carolan V and Clench MR (2010) Novel molecular tumour classification using MALDI-mass spectrometry imaging of tissue micro-array, Analytical and Bioanalytical Chemistry, 397, 587-601.
6. Groseclose MR, Massion PP, Chaurand P, Caprioli RM (2008) High-throughput proteomic analysis of formalin-fixed paraffin-embedded tissue microarrays using MALDI imaging mass spectrometry, Proteomics, 8(18):3715-24.
7. Lazova R, Seeley EH, Kutzner H, Scolyer RA, Scott G, Cerroni L, Fried I, Kozovska ME et al. (2016) Imaging mass spectrometry assists in the classification of diagnostically challenging atypical Spitzoid neoplasms, J Am Acad Dertmatol, 75(6); 1176–1186.
8. Scott DA, Casadonte R, Cardinali B, Spruill L, Mehta AS, Carli F, Simone N, Kriegsmann M, Del Mastro L, Kriegsmann J and Drake RR (2019) Increases in Tumor N-glycan Polylactosamines Associated with Advanced HER2 Positive and Triple Negative Breast Cancer Tissues, Proteomics – Clinical Applications, 13, 1800014.
9. West CA, Wang M, Herrera H, Liang H, Black A, Angel PM, Drake RR and Mehta AS (2018) N-linked glycan branching and fucosylation are increased directly in hepatocellular carcinoma tissue as determined through in situ glycan imaging, Journal of Proteome Research, 17, 10, 3454-3462.
Alice Ly completed her PhD in Anatomy, Diabetes, Neuroscience and Retina at the University of Melbourne in 2010, and held a post-doctoral research associate position at Helmholtz Zentrum München, where she became familiar with molecular tissue analysis and state of the art imaging techniques. She joined Bruker Daltonics in 2016 as a Research Scientist in MALDI Mass Spectrometry Imaging and is now R&D Manager for the MALDI Tissuetyper.
Lab Asia 33.4 - August 2026



.jpg)










-(1).jpg)

.jpg)