Laboratory events news
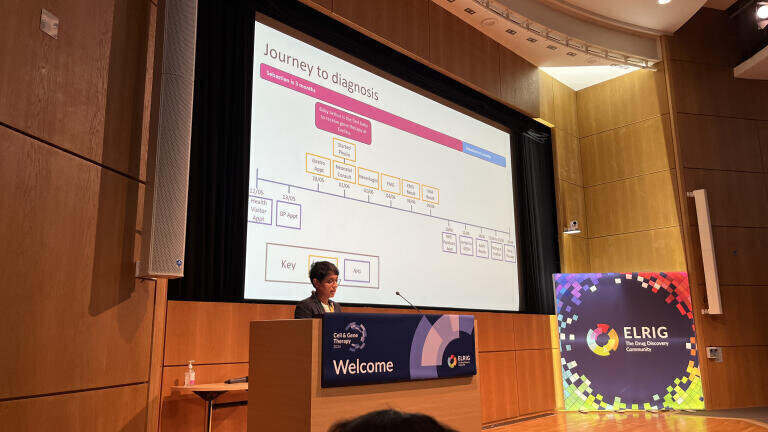
Parent advocate Mrs Dharmisha Stezaly speaking at ELRIG in March 2026 set out how early treatment with the gene therapy Zolgensma changed the course of her son Sebastian’s life after a diagnosis of spinal muscular atrophy Type 1 and highlighted why families still need rapid diagnosis and, crucially, a screening programme for newborns
Mrs Dharmisha Stezaly’s powerful presentation put a human face to one of the most important shifts in rare disease care in recent years, as she described what it has meant to secure her child, Sebastian, who has spinal muscular atrophy Type 1 (SMA1) early access to a life-altering gene therapy.
Speaking as a parent advocate, she centred her talk on the experience of accessing the gene therapy Zolgensma in 2021 when her son was only five months old and used their story to show both the remarkable potential of early intervention and the substantial burden that can still fall on families despite relatively early treatment.
Stezaly’s account combined lived experience with clinical context and striking practical detail. Her home video footage of Sebastian’s progress following his treatment gave the presentation an emotional force but the substance of the talk lay in sober analysis. Gene therapy, she showed, can alter the course of SMA1 profoundly, yet it does not remove the need for sustained, carefully coordinated and highly specialist care. In that respect, her presentation offered both a personal testimony and a wider critique of how health systems diagnose, treat and support children with severe neuromuscular disease.
Stezaly explained that Sebastian had been diagnosed with SMA1 at around four months of age. He then received Zolgensma a month later. She set the outcomes in his case against the natural history of untreated SMA1, a condition long associated with severe muscle weakness, rapid loss of function and serious threats to breathing, swallowing and death in infancy. Before the arrival of disease-modifying therapies, many families faced this bleak outlook. But her presentation made clear that this landscape has changed dramatically in just a decade.
Even so, she avoided any suggestion that Zolgensma represented a cure. One of the strongest points in the presentation was her insistence that the therapy changes prognosis but does not erase disease. She referred to the three disease-modifying treatments now available for SMA and drew a distinction between repeated treatment approaches of two other therapies XXX and XXX against Zolgensma’s one-off administration. These therapies, she explained, aim to preserve function and slow or halt deterioration by addressing the underlying biology of SMA1. But what they cannot do is restore motor neurons that have already been lost. That biological reality underpinned the harsh logic of her whole talk. In SMA1, time is not just important, it is decisive.
Her presentation repeatedly emphasised the need for faster diagnosis and routes to treatment. Stezaly described Sebastian’s diagnosis as rapid, in the end, but alarmingly fragile. She had first become concerned when he seemed unusually floppy and did not show the head control or physical development to be expected at his age. Her concerns were not immediately interpreted as signs of a serious neuromuscular disorder. Instead, she encountered a sequence of clinician’s reassurances and delays that – in a condition such as SMA1 – can carry serious long-term consequences.
She recalled how her unease persisted and how she continued to push for further assessment. Her persistence and willingness to challenge initial conclusions played a major part in what happened next. Before SMA1 was suspected by doctors, she had already begun to think that its diagnosis explained Sebastian’s symptoms and so she asked the question directly. Once that possibility came into view, the tone of the clinical journey changed sharply. The window in which treatment might protect motor function was narrow, and every day counted.
Her account of this period carried two messages at once. First, Sebastian was fortunate. He moved from confirmed diagnosis to treatment at unusual speed for a symptomatic infant in the UK’s National Health Service (NHS) which has not adopted universal newborn screening for SMA1. Second, that speed had depended too much on chance, persistence and informal acceleration rather than on a predictable pathway. She made clear that her family saw the right professionals at the right moments and had to press hard for action to be taken. It was a picture painted of a system that was not robust but rather of a family who fortunate enough to succeed despite the apparent structural weaknesses of the NHS.
Stezaly also outlined the practical realities of Sebastian having received Zolgensma. Access to treatment required extensive pre-infusion testing, including blood tests and checks on organ function, with particular attention to the liver. She explained that this was necessary because gene therapy carries risks that require close supervision. She also referred to steroid use and careful follow-up after treatment in order to manage immune and hepatic complications. This part of her story was especially important because it countered any simplistic notion of gene therapy as a single transformative moment after which ordinary life resumes. Instead, the therapy opened a further phase of medical oversight, one that depended on defined specialisms, key infrastructure and monitoring at six-month intervals.
But the visual centrepiece came from videos Stezaly shared that showed Sebastian at different stages of his development following treatment. These clips documented changes in posture, movement and mobility, offering documentary evidence of functional gains. Stezaly used this material to demonstrate the effect of gene therapy on motor development, strength and quality of life. Yet she handled this carefully. The point was not to imply that his SMA1 had vanished, but to show that intervention had redirected Sebastian’s life. The distinction matters given that therapy changed what was possible but did not make the disease irrelevant.
From there, Stezaly described a broad multidisciplinary package of support, including physiotherapy, occupational therapy, hydrotherapy, speech and language therapy, dietetic input, orthotics and specialist surgery. Some of this support came through the NHS but some required private payer supplementation. Her point was plain. Because Sebastian had already lost substantial motor function by the time he received treatment, rehabilitation remained essential in order to maximise function, support development and help him build skills that untreated progression would otherwise have been denied to him by SMA1.
She gave particular emphasis to musculoskeletal complications, especially hip pathology and scoliosis. These problems, she suggested, reflect one of the less discussed consequences of therapeutic progress in SMA1. Children who survive longer and function better now encounter orthopaedic issues that might previously have been overshadowed by its more immediate medical threats.
Sebastian underwent major hip surgery which she described as reconstructive in scope and intended to improve both comfort and function. A specialist braced for his back has been required – built to order in Chesterfield, UK – and its use for spinal management also formed part of the wider care picture. Long-term supportive care remains central even after his successful gene therapy intervention.
Stezaly further argued that access to the best possible care still depends too heavily on where a family lives, what they know or can learn quickly, how hard they can push and whether they can afford to fill gaps in treatment care with private funding. She described how accessing social media groups and their international patient communities had helped her locate expertise, compare health provider approaches and identify options that formal care pathways had not always made visible. While she spoke positively about the value of these networks, she also used their importance to expose a systemic problem. Families should not need extraordinary resourcefulness in order to secure appropriate care for a child with severe disease even if it is rare.
This part of her experience flowed directly into one of the strongest policy conclusions of her talk which is the burning case for newborn screening. Stezaly argued that the NHS introducing newborn screening would reduce diagnostic delay, permit treatment before irreversible neuronal loss and improve both outcomes and – in the long-term – cost-effective lifetime treatment burdens to payers. She contrasted Sebastian’s relatively positive trajectory with the much heavier burden that can follow a later diagnosis and its consequent later intervention, including hospital admissions, respiratory support, transport demands and complex long-term care packages. Her case was therefore both clinical and economic by showing that earlier diagnosis would not only protect function for the individual but also reduce downstream spending by healthcare service providers. She detailed a number of European peer nations that already had newborn in place and highlighted that even Ukraine has adopted screening as standard practice during it period of war with Russia since 2022.
Stezaly further argued that policy debates about value, evidence and access must take fuller account of lived experience. Cost-effectiveness models and data collection exercises can miss crucial elements of family life, including parental mental health, employment disruption (and hence reductions in national taxation receipts), the challenge of fragmented services and the constant need to negotiate accessibility in ordinary settings. She made the point that these realities are not peripheral to treatment decisions. They form part of the true cost of disease and the true value of timely intervention.
At the same time, her account retained warmth and perspective. Sebastian emerged from the presentation not as an abstract case study but as a lively and determined child whose life has been sustained by treatment and enlarged by relentless care.
Stezaly showed that scientific progress has opened possibilities that would once have seemed unreachable while making clear that no drug – no matter however sophisticated – can substitute for early diagnosis, coordinated support and a health system prepared to listen to families.
Taken together, Stezaly’s presentation amounted to far more than a personal success story. It was a serious argument about what it takes to turn a breakthrough therapy into meaningful, durable benefit. In Sebastian’s case, Zolgensma changed the trajectory of a devastating condition. Yet the broader lesson was that treatment alone is not enough. Children with SMA1 and their families still need fast diagnosis, comprehensive follow-up, specialist rehabilitation, equitable access to services and policymaking that values lived experience as highly as clinical metrics. On a final note of hope, an ELRIG delegate broke the news that the NHS in Scotland was about to adopt newborn screening.
Lab Asia 33.4 - August 2026



.jpg)









-(1).jpg)

.jpg)