Research news
Intensive low-density lipoprotein cholesterol reduction with evolocumab has been shown to cut first major cardiovascular events in patients with high-risk diabetes but no established atherosclerosis, with findings that may reshape primary prevention strategies
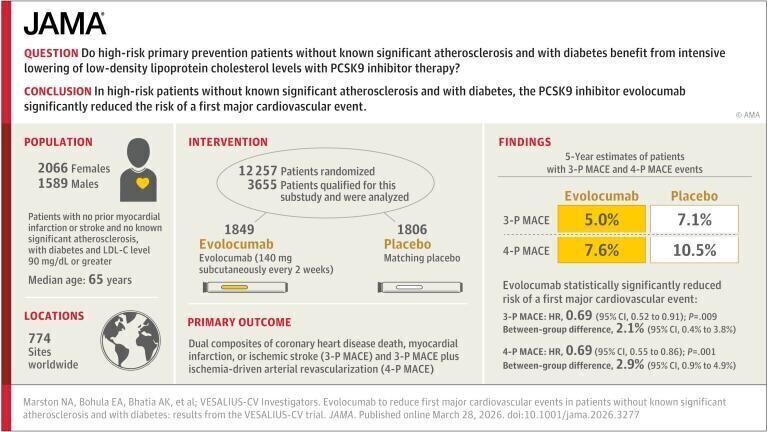
Researchers have reported that intensive lowering of cholesterol with evolocumab cut the risk of a first major cardiovascular event in high-risk type-2 diabetes (T2DM) patients who did not have known atherosclerotic disease. The findings were presented by a team from Mass General Brigham hospital, Boston, Massachusetts, USA, at the American College of Cardiology Annual Scientific Session at the end of March 2026, held in Chicago, Illinois, USA.
Cardiovascular disease remains the leading cause of death worldwide and strategies to reduce risk have focused heavily on lowering serum concentrations of low-density lipoprotein (LDL) cholesterol – often referred to as ‘bad cholesterol’. Evolocumab is a monoclonal antibody that inhibits the proprotein convertase subtilisin kexin type 9 and has been established as a potent lipid-lowering therapy capable of reducing LDL cholesterol by approximately 60 per cent. This effect adds to that which can be achieved by using statins which remain standard of care for most patients at elevated cardiovascular risk.
Historically, intensive cholesterol-lowering approaches such as those based on proprotein convertase subtilisin kexin type 9 inhibition have been reserved largely for patients with established cardiovascular disease. By contrast, patients without diagnosed atherosclerosis but with elevated risk have typically received statins alone, and in some cases no pharmacological lipid-lowering therapy at all.
In a prespecified subgroup analysis of the VESALIUS-CV randomised trial – sponsored by the biotech giant Amgen – investigators assessed whether evolocumab could prevent cardiovascular events in a cohort of 3,655 patients with high-risk T2DM but without clinically evident atherosclerosis.
High-risk T2DM was defined rigorously as disease of at least 10 years’ duration, or requiring daily insulin therapy, or associated with microvascular complications such as retinopathy, nephropathy or neuropathy. These criteria identify a population with substantial vascular risk despite the absence of overt plaque burden detectable through conventional clinical assessment.
Participants received either evolocumab administered by subcutaneous injection every two weeks or a matched placebo. All patients continued to receive standard lipid-lowering therapy, which included statins and, where appropriate, ezetimibe. This design allowed investigators to isolate the incremental benefit of adding evolocumab to contemporary background therapy.
The lipid-lowering effect observed during the trial was pronounced. After 48 weeks of treatment, median LDL cholesterol concentrations were approximately 51 per cent lower in the evolocumab group compared with placebo, with levels of 52 milligrams per decilitre versus 111 milligrams per decilitre, respectively. These reductions are consistent with the known pharmacodynamic profile of proprotein convertase subtilisin kexin type 9 inhibitors and confirmed that substantial lipid lowering can be achieved even in patients already receiving standard therapy with statins and/or ezetimibe.
Clinical outcomes mirrored biochemical testing with a median follow-up period of nearly five years showing that patients treated with evolocumab – in addition to standard therapy – experienced a 31 per cent reduction in the risk of a first major cardiovascular event compared with those who received standard therapy alone.
The composite endpoint included death from coronary heart disease, myocardial infarction or ischaemic stroke. At five years, event rates were 5 per cent in the evolocumab group compared with 7.1 per cent in the placebo group, an absolute difference that is clinically meaningful in a primary prevention population.
Safety findings supported the tolerability of the intervention with serious adverse events occurring at similar rates in both treatment arms, indicating that the addition of evolocumab did not introduce a significant safety burden in this cohort. This observation is particularly relevant in a primary prevention setting, where the threshold for acceptable risk is typically lower than in patients with established disease.
“These results demonstrate the benefit of intensive lowering cholesterol earlier and should change how we think about the prevention of heart attacks, strokes, and heart disease in patients without known significant atherosclerosis,” said Dr. Nicholas A. Marston, cardiologist at the Mass General Brigham Heart and Vascular Institute and corresponding author of the study.
“For more than a decade, the most intensive cholesterol lowering has been reserved for patients who already have cardiovascular disease,” he added.
The findings have important implications for the conceptual framework of cardiovascular prevention. They suggest that aggressive lipid lowering may confer substantial benefit even before the clinical manifestation of atherosclerosis, particularly in metabolically high-risk populations such as those with long-standing or complicated T2DM. This challenges the traditional dichotomy between primary and secondary prevention and raises the prospect of a more graduated, risk-based approach to lipid management.
The investigators have noted that further studies will be necessary to determine whether similar benefits extend to other high-risk groups without established atherosclerosis. Such populations may include individuals with chronic kidney disease, genetic lipid disorders, or combinations of metabolic risk factors that confer elevated cardiovascular risk despite the absence of detectable plaque.
If confirmed, these results may prompt reconsideration of treatment guidelines and reimbursement frameworks, particularly given the cost associated with proprotein convertase subtilisin kexin type 9 inhibitors. The balance between clinical benefit, economic considerations and long-term population health outcomes will require careful evaluation.
For now, the VESALIUS-CV subgroup analysis provides robust evidence that earlier and more intensive intervention on lipid levels can reduce the incidence of first cardiovascular events in a clearly defined high-risk population. It reinforces the central role of LDL cholesterol in atherogenesis and supports the principle that earlier intervention may yield greater cumulative benefit over time.
For further reading please visit: 10.1001/jama.2026.3277
Lab Asia 33.4 - August 2026



.jpg)









-(1).jpg)