
News
Researchers at Washington University School of Medicine in St. Louis have identified metabolite signatures in post-operative breast fluid that have predicted implant-related infection days to weeks before clinical symptoms appear, a finding that could support earlier treatment, reduce implant loss and outcomes post- breast reconstruction
In the USA, one in eight women will receive a breast cancer diagnosis during their lifetime and about half of those patients will undergo mastectomy. Many then choose surgical breast reconstruction, most often with implants. Yet implant-based reconstruction has carried a substantial infection risk in a notable minority of patients with frequent severe consequences.
When infection has taken hold, treatment has typically required intravenous antibiotics and – in many cases – implant removal. That clinical pathway has increased the likelihood of further procedures, has delayed aspects of cancer care and has added both financial pressure and emotional strain at a time when patients have already faced the often harsh physical and psychological demands of cancer treatment.
Researchers at Washington University (WashU) School of Medicine in St. Louis, Missouri, USA, have now reported a potentially important route for earlier intervention. Their study has identified molecular signals in fluid collected after reconstruction that have indicated likely infection before visible clinical signs emerged. The work has raised the prospect of routine surveillance that could allow clinicians to treat high-risk patients sooner, with a better chance to preserve implants and to avoid escalation in need for additional care.
The research team, led by Dr. Jeffrey P. Henderson, professor in the John T. Milliken department of medicine at WashU, has focused on biomarkers detectable in post-operative fluid from reconstructed breasts. The investigators reported that these markers appeared days – and in some cases weeks – before typical symptoms of redness, swelling or inflammation would normally be a trigger for clinical concern.
This interval matters because conventional diagnosis has depended heavily on signs that can emerge late and can also resemble expected post-surgical tissue responses, which has made early discrimination difficult in routine practice.
“The ability to identify with a molecular signature early … that a patient will go on to have an infection opens up the possibility of surveillance as part of standard care,” said Henderson.
“This has the potential to enable earlier treatment that would be far more effective – and potentially curative – in patients who would otherwise progress to prolonged courses of treatment and surgery, or even implant removal and reconstructive failure,” he said.
Dr. Margaret A. Olsen, a retired professor of medicine in the division of infectious diseases at WashU and co-author of the paper, had observed high infection rates among patients who had implant-based reconstruction after mastectomy. That concern prompted further collaboration with plastic and reconstructive surgeons at the institution, who identified a central unmet need in direct terms in that clinicians needed a clear test with actionable output to indicate whether infection was likely to develop.
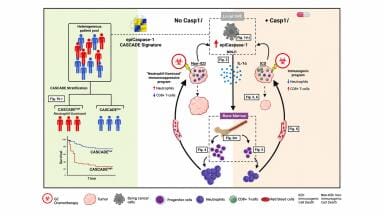
To address that need, Henderson and lead author Dr. John A. Wildenthal, at WashU, applied a metabolomics methods. Metabolomics is the analysis of small molecules, known as metabolites, that reflect ongoing biochemical activity in tissues and fluids. In infection, these molecules can capture signals from two sources at once:
Because of that dual biological readout, metabolite patterns can provide an earlier and more specific signal than late clinical signs alone.
The team worked with WashU surgeons to collect fluid samples from 50 volunteer patients across routine post-operative follow-up visits. The cohort included women who later developed infection after post-mastectomy implant reconstruction and women who did not. Investigators then compared metabolite profiles between the two groups and identified molecular patterns strongly associated with subsequent infection. Importantly, some signatures appeared well before symptoms became clinically evident.
The authors also reported that certain metabolite combinations were associated with more severe infection trajectories, suggesting the possibility not only to detect risk early but also to stratify likely severity and tailor treatment intensity.
“Originating from clinical intuition and validated through a clinical study, the evidence in this paper now supports proactive, targeted interventions to predict and address infections before they become clinically significant,” said Dr. Justin M. Sacks who is the ‘Sydney M. Shoenberg Jr. and Robert H. Shoenberg’ Endowed Chair in Plastic and Reconstructive Surgery, and director of the division of plastic and reconstructive surgery at WashU and co-author on the study.
“Such interventions can substantially reduce the burden of complications, implant loss and reconstructive failures in these patients,” he added.
From a clinical workflow perspective, the researchers suggested a practical translation pathway. A future point-of-care assay could potentially fit within routine post-operative reviews, where fluid assessment and targeted decision-making could occur without major disruption to standard care pathways. Dr. Terence M. Myckatyn, professor of surgery at WashU and co-author who treats breast cancer reconstruction patients, described how such a tool could sharpen antibiotic use and improve stewardship.
“If the test is positive, antibiotics can be started pre-emptively in these select patients to thwart infection,” said Myckatyn.
“And perhaps just as important, we would not give antibiotics to those with a negative test, thereby adhering to a thoughtful approach for antibiotic stewardship,” he said.
That distinction has particular relevance as healthcare systems continue to expand stewardship programmes to more effectively manage the mounting pressures of antimicrobial resistance. A test that can identify high-risk patients earlier could help clinicians act faster where benefit is likely, while avoiding unnecessary antibiotic use, prophylactically, where risk remains low. In other words, the same diagnostic signal could support two quality goals at once, on one hand better patient outcomes and on the other more selective and responsible prescribing.
Validation studies will be needed to confirm reproducibility across broader and more diverse patient populations – and different surgical settings –before any assay can enter widespread use. If validation is positive, the development of a prospective clinical diagnostic tool could follow. The broader scientific value may also extend beyond breast reconstruction. Because the work has mapped metabolomic features of tissue infection in humans, it could inform future strategies to classify and treat other post-surgical infections with greater precision which could reveal candidate biological pathways elsewhere for therapeutic targeting.
“While better techniques are always being sought, the reality is that infections still occur despite a meticulous surgical approach,” said Myckatyn.
“To be able to identify biomarkers that can portend an infection days before it develops is huge,” he concluded.
Taken together, the study has offered a clinically grounded model for earlier intervention in a common complication that exacts high personal and healthcare burdens. If subsequent validation confirms these findings, metabolite-guided surveillance could become a meaningful addition to post-mastectomy reconstruction care – one that improves the chance to preserve reconstruction, reduce treatment burden and support recovery with fewer setbacks.
For further reading please visit: 10.1172/JCI192104
ILM Guide 2026/27

.jpg)



















2.jpg)
