Clinical, medical and diagnostics
Researchers at Nagoya University have reported that ovarian cancer cells form hybrid clusters with mesothelial cells in abdominal fluid, a process that appears to accelerate tissue invasion and strengthen chemotherapy resistance. The findings have offered a mechanistic explanation for fast peritoneal dissemination
Ovarian cancer remains the deadliest gynaecological malignancy, with many patients receiving diagnosis only after widespread dissemination across the abdominal cavity. That clinical pattern has posed a central question which is why this disease progresses with speed before detection pathways can identify it. A study led by Nagoya University, Nagoya, Japan, has provided a detailed cellular explanation and has shifted attention towards a previously underappreciated pathway for metastatic spread.
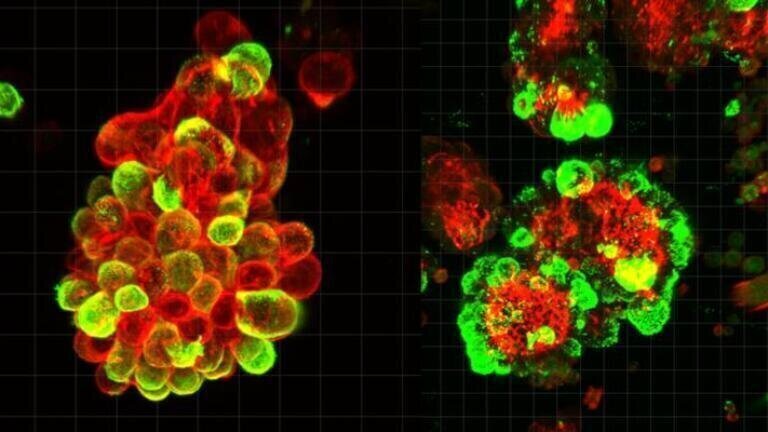
The investigators reported that ovarian cancer cells in ascitic fluid did not usually travel as isolated malignant cells. Instead, they frequently attach to mesothelial cells, which normally line and protect the peritoneal cavity, forming multicellular hybrid spheres. In patient-derived samples, approximately 60 per cent of observed cancer spheres contained mesothelial cells. That proportion suggested that hybridisation was not a rare event but a common biological occurrence.
Ovarian cancer cells release transforming growth factor beta 1 (TGF-β1) and this signal altered mesothelial cell behaviour. In response, mesothelial cells developed protrusive, spike-like invasive structures – invadopodia – that enabled penetration through surrounding tissue barriers. In functional terms, mesothelial cells appeared to cut the path with the cancer cells moving through the resulting openings.
This mechanism addressed a long-standing gap in understanding the peritoneal phase of ovarian cancer spread. In many solid tumours, including breast and lung cancer, malignant cells enter blood vessels and travel through these comparatively defined circulatory routes. By contrast, ovarian cancer has often spread transcoelomically, with cells detaching from the primary tumour and dispersing through peritoneal fluid, which has no fixed vascular architecture. Respiratory motion and routine body movement can redistribute that fluid across abdominal surfaces, exposing multiple anatomical sites to metastatic seeding. The interval between detachment and re-attachment has therefore represented a critical yet poorly characterised window in disease progression.
The Nagoya team has now characterised that interval as an active co-operative stage rather than a passive drift phase. Their imaging work showed that mesothelial and cancer cells adhered to each other in suspension, then arrived at distant peritoneal sites as organised clusters with enhanced invasive capacity. Importantly, those hybrid spheres also showed stronger resistance to chemotherapy than spheres that contained only malignant cells which may help to explain why standard cytotoxic regimens can fail to prevent recurrence in advanced disease.
The researchers analysed ascitic fluid from patients with ovarian cancer, used advanced microscopy to track cell behaviour in real time, validated key observations in mouse models, and applied single-cell genetic analysis to resolve cell-state changes within mixed populations. That multi-platform strategy strengthened the study’s central claim that mesothelial recruitment was functionally relevant and not merely coincidental.
“They manipulate mesothelial cells to do the tissue invasion work,” said lead author Dr Kaname Uno, a visiting researcher at Nagoya University Graduate School of Medicine.
“They undergo minimal genetic and molecular changes and just migrate through the openings that mesothelial cells create,” he said.
His description suggested a tactical economy in which malignant cells outsource physically demanding invasion steps rather than extensively reprogramme themselves at each stage.
Dr Uno’s had practised as a gynaecologist for eight years before he moved into full-time research. He said that one patient’s course proved decisive in that transition from the clinic to the research bench. In that case, despite clear screening findings only three months earlier, the patient later presented with advanced ovarian cancer that contemporary tools failed to detect soon enough for curative intervention. That case has underlined a persistent challenge in the field, where biological aggressiveness can outpace surveillance intervals and currently available biomarkers.
Current chemotherapy protocols primarily target malignant cells, yet this work has indicated that non-malignant stromal partners can materially influence invasion efficiency and treatment resistance. If mesothelial co-operation proves necessary for rapid dissemination in broader cohorts, then treatment paradigms may need to expand from tumour-cell-centric models to ecosystem-level intervention.
The first is pathway is to effect interruption whereby therapeutic strategies could attempt to block TGF-β1-mediated signalling that converts mesothelial cells into invasion facilitators. The second is structural disruption such that interventions could seek to prevent formation or persistence of hybrid spheroids in ascitic fluid before implantation at secondary sites. Either approach would however act as a complementary treatment regimen – rather than replace – tumour-directed cytotoxic therapy.
Given that hybrid clusters were detectable in abdominal fluid, serial assessment of cluster prevalence or phenotype could support risk stratification, early recognition of aggressive progression, or response evaluation during treatment. In principle, ascites-based cellular profiling could add clinically useful information where imaging or serum markers provide incomplete resolution of active dissemination dynamics.
Preclinical validation in animal models and cellular systems has supported the mechanism but prospective clinical studies must still test whether targeting this axis improves survival, delays recurrence, or changes surgical outcomes in practice.
It will also be important to determine whether this mechanism operates similarly across ovarian cancer subtypes and treatment histories, including platinum-sensitive and platinum-resistant disease contexts.
Even with those caveats, the work has reframed a central biological problem in ovarian oncology. The study has suggested that rapid abdominal spread does not rely solely on increasingly aggressive cancer cell clones. Instead, malignancy may exploit host mesothelial biology to accelerate invasion while retaining relative molecular stability in tumour cells themselves. That insight has practical force because it points to intervention points that existing regimens have largely overlooked.
For clinicians and researchers, the message is direct. Ovarian cancer dissemination in the peritoneal cavity appears to involve organised intercellular collaboration, not random cellular shedding alone.
For further reading please visit: 10.1126/sciadv.adu5944
ILM 51.5 July 2026


.jpg)









-(1).jpg)