Laboratory events news
Researchers have reported that the widespread use of glucagon-like peptide-1 receptor agonists – prescribed for diabetes and weight management treatment – may alter tracer uptake on oncological PET-CT imaging, creating patterns that risk misdiagnosis
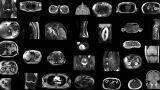
The widespread use of glucagon-like peptide-1 (GLP-1) receptor agonists may complicate the interpretation of oncological fluorodeoxyglucose positron emission tomography–computed tomography (FDG PET-CT) scans, according to research presented at the 38th Annual Congress of the European Association of Nuclear Medicine.¹
GLP-1 receptor agonists have been prescribed widely to individuals with both type 2 diabetes and to those for whom weight loss is of clinical benefit. Uptake in the United States has been reported to rise by 700 per cent between 2019 and 2023.²
These therapies alter glucose metabolism, gastric motility and sympathetic nervous system activity. As a result, they can influence patterns of fluorodeoxyglucose uptake during PET-CT imaging. Case reports have already been documented of heightened uptake in skeletal muscle, the myocardium and brown adipose tissue, all of which could be mistaken for evidence of malignant disease or inflammatory processes.³,⁴
A retrospective case series conducted by Alliance Medical Ltd. examined FDG PET-CT scans in patients taking GLP-1 receptor agonists. The investigators reported several atypical patterns of tracer uptake that could readily be misclassified as pathological in the absence of a full record of the patient’s treatment regimen.
“We noticed an unusual uptake in one of our patients on a GLP-1 agonist which prompted a wider review across our network,” explained lead author Dr Peter Strouhal, Medical Director at Alliance Medical Ltd, in the United Kingdom.
“We found that these altered patterns are increasingly common, yet there is currently no national or international guidance in the UK addressing this emerging issue.”
Such misinterpretations have the potential to trigger additional and unnecessary diagnostic investigations, to distort staging decisions in cancer, and to delay the initiation of appropriate therapies. This, in turn, may heighten patient distress and generate potentially avoidable uncertainty.
“Recognising the characteristic uptake associated with GLP-1 agonists helps to avoid unnecessary anxiety and interventions, ensure patients receive the right care at the right time,” Dr Strouhal added.
The research team emphasised that they do not, at present, recommend any change to patient preparation protocols or the discontinuation of GLP-1 therapy prior to FDG PET-CT examinations. Instead, they urged imaging teams to obtain and record comprehensive medication histories for each patient in order to support correct interpretation while formal guidance evolves.
Although the UK has not yet issued any guidance, Australia recommends advising patients to continue treatment, but to fast from midnight before their scan, to undergo imaging in the morning and to maintain good glycaemic control.⁵
References:
Strouhal P, Meadows A, McGovern A. A Weighty Problem: GLP-1 Agonists and the Altered Images of FDG PET-CT. Presented at EANM'25 on Wednesday 8 October 2025.
Mahase E. GLP-1 agonists: US sees 700% increase over four years in number of patients without diabetes starting treatment. (2024.) BMJ.
Oldan JD, Landman PG, Schroeder JA et al.(2024). FDG PET in a Patient on a GLP-1 Agonist/Insulin Secretagogue. Clinical Nuclear Medicine.
Harrison DB, Phillips AL, Tansey JB et al. (2025). Brown Adipose Tissue Mimicking Head and Neck Cancer on PET Scan in a Patient on GLP-1 Drug. Laryngoscope. PubMed. National Library of Medicine.
Greenfield J, Mikaheal Y and Ludington J. (2024). Joint ADS/ANZSNM guideline for FDG PET/CT imaging in patients with type 1 and type 2 diabetes. Australian Diabetes Society & ANZSNM.
ILM 51.5 July 2026












-(1).jpg)
.jpg)


.jpg)